

Coronary bypass surgery, widely used to treat cardiovascular disease, involves redirecting a patient’s bloodflow around the heart in order to allow surgeons to operate. Heart-lung machines synthetically oxygenate and pump blood during such surgeries in order to keep the patient alive. The first heart-lung machine dates back to the 1930s and consisted of many of the same components as the machines of today. The design of each of these components is inspired by different principles of physics and engineering, including fluid dynamics and pressure gradients. Engineers are now applying these same concepts to create new heart-lung machine models such as miniaturized or portable versions. With its foundations in biology, physics, and engineering, the heart-lung machine has proven to revolutionize the treatment of heart disease.
Introduction
Heart disease is a major health problem facing Americans today. According to the American Heart Association, 80 million men and women suffered from cardiovascular disease in 2006. In 2005, over 860,000 cardiovascular disease patients died [1]. Despite these statistics, the situation is not hopeless. Different solutions exist, such as lifestyle changes, medicines, or in the most severe cases, coronary bypass surgery. Patients can undergo different types of cardiac bypass surgery to repair their faulty hearts or blood vessels. The surgery is commonly referred to as open heart surgery because the doctors actually open up the patient’s chest cavity, expose the heart, and operate on it. In order to allow such a surgery to be performed, the heart must be temporarily stopped from beating.
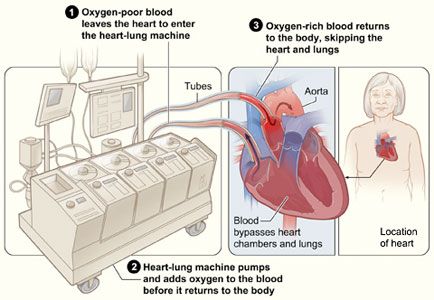
Obviously the heart is an essential organ. If it stops beating, oxygen-carrying blood cannot be circulated through the body, and a person will die shortly afterward. This presents quite a predicament for cardiovascular surgeons: how can they stop the heart to operate on it, yet keep the patient alive? The answer lies with a special apparatus, called the heart-lung machine, or cardiopulmonary bypass machine. The heart-lung machine is a device that is connected to the blood vessels and serves as the person’s heart and lungs for a period of time. In other words, the patient’s blood bypasses the heart to enter the machine instead, where it is oxygenated just as it would be in the lungs. From there, the machine pumps the blood out into the rest of the body (Fig. 1).
In doing so, the heart-lung machine essentially replaces the most vital organs, thereby sustaining the patient’s life. From its original development to the components of current models to its future applications, the heart-lung machine is truly an impressive feat of technology that integrates the engineering principles of fluid flow, pressure gradients, and heat transfer into one life-saving device.
History of the Heart-Lung Machine
The first machine of this type was developed by surgeon John Heysham Gibbon in the 1930s [2]. During this time, physicians were looking into the possibility of extracorporeal circulation, or blood flow outside of the body [3]. They wondered if there was a way to extend this extracorporeal circulation to bypass not just minor organs, as was often done in surgery at the time, but to bypass the heart completely. Saddened at a patient’s death mid-surgery, Gibbon made it his mission to come up with an artificial heart-lung machine that would keep a patient alive during heart surgery.
Between 1934 and 1935, Gibbon built a prototype of his heart-lung machine and tested its function on cats in order to assess what problems needed to be addressed before using it with humans [4]. For example, in one model Gibbon observed that an inadequate amount of bloodflow was exiting the machine, so he decided to make the flow continuous, instead of in short pulses [4]. By introducing bloodflow that would remain at the same rate continuously, instead of increasing and decreasing with a set rhythm, he increased the total blood volume capacity that could flow throughout the machine.
In the 1940s, Dr. Gibbon met Thomas Watson, an engineer and chairman of International Business Machines (IBM). Gibbon and Watson, along with other engineers from IBM, collaborated on the quest for an effective cardiopulmonary bypass machine, and together they created another new model [2]. When this model was testing by performing surgeries on dogs, they noticed that many of their test subjects died after surgery due to embolisms (An embolism occurs when a small particle or tissue migrates to another part of body and causes the blockage of a blood vessel, which prevents vital tissues from receiving oxygen) [5]. From these experiments, they saw the need to add a filter to their apparatus. Gibbon and the IBM engineers decided to use a 300-micron by 300-micron mesh filter, which proved successful in trapping these harmful tissue particles [4].
In 1953, Gibbon himself completed the first successful surgery on a human patient with the help of the cardiopulmonary bypass machine [6]. Since then, open heart surgeries have been performed for over 55 years, with almost 700,000 performed annually in recent years [1]. Much has changed since Gibbon’s first model, but the main engineering concepts behind his machine have remained the same. Today’s heart-lung-machine contains the same basic components: a reservoir for oxygen-poor venous blood, an oxygenator, a temperature regulator, a pump to drive the blood flow back to the body, a filter to prevent embolisms, and connective tubing to tie all the other elements together [4].
Today’s Machine: A Journey Through its Components
In an open-heart surgery, the surgeon first connects the bypass machine to the patient by inserting tubes called the venous cannulas into the vena cavae, the large blood vessels leading to the heart [7]. This redirects the flow of blood into the heart-lung machine, bypassing the heart completely. Engineers must design the venous cannulas such that a precise and controlled amount of blood will flow through them into the machine. They do so by creating the tubes in varying sizes and resistances [8]. According to fluid dynamic principles, the larger a tube is, the more liquid can flow through it at a given point in time. On the other hand, if a tube has a greater resistance, which is controlled by surface roughness and fluid viscosity, then less fluid may pass through. By adjusting these two properties, an engineer can create venous cannulas that allow specific rates of blood to flow from the body and into the machine.
From the cannulas, the blood flows into the venous reservoir, a chamber made of plastic or polyvinyl chloride (PVC) that collects and stores the blood from the patient’s body [9]. The reservoir must have a large volume capacity to accommodate a large volume of blood. According to Boyle’s Law, pressure and volume are inversely related under constant temperature; as one increases, the other decreases. Thus, the venous reservoir’s large volume gives it a low pressure. All solvents naturally move from regions of higher pressure to regions of lower pressure. Therefore, since the reservoir has a low pressure, blood flows from the high-pressure vessels in the body into the bypass machine’s venous reservoir.
Upon leaving the venous reservoir, blood next travels into the heart-lung machine’s pump, which utilizes compression force or centrifugal force to drive blood flow. A pump may come in either one of two types: roller pumps or centrifugal pumps. In a roller pump, the blood enters a curved track of tubing made of a flexible material, often PVC, latex, or silicone [8]. As the blood enters, two cylindrical rollers rotate and slide forward, constricting the tubing. This compression reduces the volume in the tube, giving the blood no room to go but forward. Just as squeezing a tube of toothpaste pushes the paste forward and out of the tube, compressing the roller pump forces the blood to flow forward, through the rest of the bypass machine. While roller pumps may be used as the primary pump in a heart-lung machine, centrifugal pumps are often used as an alternative. The centrifugal pump is comprised of a plastic wheel that rotates rapidly, propelling the liquid away from the center of rotation [8]. Imagine spinning a bucket of water overhead fast enough so that water is pressed outward against the bucket and does not fall out. The same force is utilized in the heart-lung machine as the rotation of the centrifugal pump forces the blood to flow past the spinning wheel and out towards the next section of tubing. While some heart-lung machine manufacturers prefer this type of pump because they believe it reduces the formation of harmful clotting elements in the blood, at this point in time, both types of pumps are widely used [10].
Blood flows from the pump into the heat exchanger, which uses the concept of heat transfer to cool the blood down to the optimal temperature for surgery. The human body normally maintains an internal temperature of 37 degrees Celsius but during cardiac surgery, physicians lower the patient’s core temperature to a state of moderate hypothermia or 5 to 10 degrees lower than usual [8]. Oxygen gas is more soluble in cold blood than in warm blood [11]. Thus, lowering the temperature maximizes the amount of oxygen the patient’s blood cells can carry.
Following the basic principle of heat transfer, a warmer object will always transfer heat to any colder object with which it is in contact. Similarly, if a cold object touches a warmer object, the warmer object will be cooled. That is precisely what occurs in the heart-lung machine’s heat exchanger. It consists of a thermally adjustable compartment of cold water with plastic rubes submerged in it. As blood flows through the tubes, thermal energy is transferred between the water and the tubing, and then between the tubing and the blood. The warmer object, the blood, becomes colder, while the cooler object, the water, becomes warmer. Thus, the heat exchanger cools the blood to the desired temperature.
From the heat exchanger, the cooled blood enters the oxygenator, where it is imbued with oxygen. Today’s heart-lung machines use an oxygenator that attempts to mimic the lung itself. This oxygenator, aptly called a membrane oxygenator, consists of a thin membrane designed like the thin membranes of the alveoli, the air-filled sacs that comprise the lungs. Venous blood from the heat exchanger flows past one side of the membrane, while oxygen gas is stored on the other. Micropores in the membrane allow oxygen gas to flow into the blood and into the blood cells themselves. Just as blood spontaneously flows along a pressure gradient, gases also move from regions of high pressure to regions of low partial pressure. The oxygenator is designed such that the oxygen pressure on the gas side of the membrane is much higher than the pressure in the blood [12]. Thus, oxygen passes through the membrane into the blood, following the natural high-to-low pressure gradient.
At this point in the journey through the heart-lung machine, the blood has been collected, cooled and oxygenated, so it is nearly ready to return to the patient’s body. Before this can happen, however, it must pass through a filter to eliminate the potential for embolisms. Anything that could lead to blockage of a blood vessel, whether it is an air bubble, a piece of synthetic material, or a clotting protein, poses a great risk to the patient and must be filtered out of the returning blood. The filters used in the heart-lung machine are comprised of nylon or polyester thread woven into a screen with small pores [8]. The small pores trap the harmful bubbles or particles, allowing purer blood, free from dangerous embolism-causing particles, to flow through. After being filtered, the blood travels through plastic tubes called arterial cannulas. Arteries, the blood vessels that deliver oxygen-rich blood from the heart to the rest of the body, have the highest speed of any vessel. In order to imitate this, engineers designed the arterial cannulas to be very narrow [8]. In fluid dynamics, the flow rate of a liquid through a vessel is equal to the cross-sectional area times the speed of flow. Thus, tubes like the arterial cannulas that have a smaller diameter allow for a higher blood velocity. During surgery, the physician inserts the cannulas into one of the major arteries of the patient, such as the aorta or the femoral artery [7]. Blood then leaves the last component of the cardiopulmonary bypass machine, enters the patient’s own vessels, and again makes its natural journey through the circulatory system.
Heart-Machines of the Future
There are dozens of heart-lung machines currently on the market today that are widely used in operating rooms across the nation. Most of these machines employ the same basic components and functions. However, like most areas of science and engineering, the technology of the heart-lung machine is not stagnant. Recent breakthroughs of biomedical engineers give a glimpse of the cardiopulmonary bypass machines of the future. In 2007, the world’s first portable heart-lung machine received the CE mark, which officially allowed it to be sold across Europe. Weighing only 17.5 kilograms and powered by a rechargeable battery, the Lifebridge B2T can be transported to different parts of a hospital, giving paramedics or emergency room physicians the chance to start extracorporeal circulation in critical patients before even reaching the operating room [13] (Fig. 2).

Another new development of the heart-lung machine is the MiniHLM, a miniaturized heart-lung machine developed for infants. Instead of having all the components spaced separately, as with normal-sized machines, the MiniHLM integrates the functions so the machine is much smaller and more compact [13]. This allows cardiac bypass surgery to be performed on neonates, something that will surely expand the capacity with which heart conditions in newborns can be treated.
Current implementations of the cardiopulmonary bypass machine have advanced far past John Gibbon’s original idea almost 80 years ago. Yet no step in the process has been insignificant, as every improvement has improved the safety and usability of the machine. Engineers continue to consider both the biological needs of the human body and the basic principles of physics in order to create a functional biocompatible device that performs what was once unthinkable, sustaining human life without the use of one’s heart or lungs. Hundreds of thousands of patients undergo open-heart bypass surgeries every year, intense procedures which require extracorporeal circulation [14]. That’s hundreds of thousands of lives saved with the help of one essential biomedical device: the heart-lung machine.
References
-
- [1] “AHA Heart Disease and Stroke Statistics – 2009 Update.” American Heart Association. Internet: http://www.americanheart.org/downloadable/heart/1240250946756LS-1982%20Heart%20and%20Stroke%20Update.042009.pdf, 2009. [28 Jun 2009].
- [2] “Internal Working of the Cardiopulmonary Bypass Machine.” The Chemical Engineers’ Resources. Internet: http://www.cheresources.com/ cardiopul.shtml, 2008. [29 Jun 2009].
- [3] “Extracorporeal circulation.” The American Heritage Medical Dictionary. 2007. Internet: http://medical-dictionary.thefreedictionary.com/ extracorporeal+circulation [29 Jun 2009].
- [4] Adora Ann Fou. “John H. Gibbon. The first 20 years of the heart-lung machine.” Texas Heart Institute Journal, vol. 24(1), pp. 1-8, [On-line] Available: http://www.pubmedcentral.nih.gov/pagerender.fcgi?artid=325389&pageindex=1 [29 Jun 2009].
- [5] Kelly D. Hedlund.”A Tribute to Frank F. Allbritten, Jr. Origin of the Left Ventricular Vent during the Early Years of Open-Heart Surgery with the Gibbon Heart-Lung Machine.” Texas Heart Institute Journal, vol. 28(4), pp. 292-296. [On-line] Available: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=101205, 2001 [30 Jun 2009].
- [6] Lawrence H. Cohn “Fifty Years of Open-Heart Surgery.” Circulation, vol. 107, pp. 2168-2170. [On-line] Available: http://circ.ahajournals.org/cgi/content/short/107/17/2168, 2003 [29 Jun 2009].
- [7] Ludwig K. Von Segesser. “Peripheral cannulation for cardiopulmonary bypass.” Multimedia Manual of Cardiothoracic Surgery Internet: http://mmcts.ctsnetjournals.org/cgi/content/full/2006/1009/mmcts.2005.001610, 2006, [30 Jun 2009].
- [8] Eugene A. Hessel, II, and L. Henry Edmunds, Jr. “Extracorporeal Circulation: Perfusion Systems.” Cardiac Surgery in the Adult. [On-line] New York: McGraw-Hill, Available: http://cardiacsurgery.ctsnetbooks.org/cgi/ content/full/2/2003/317 2003, [30 Jun2009].
- [9] “Venous Reservoirs.” Perfusion Equipment. Internet: http://www.perfusion.com.au/CCP/Perfusion%20Equipment/ Venous%20Reservoirs.htm, 2008, [30 Jun 2009].
- [10] Masaru Yoshikai, Masakatsu Hamada, Kyoumi Takarabe, and Yukio Okazak. “Clinical Use of Centrifugal Pumps and the Roller Pump in Open Heart Surgery: A Comparative Evaluation.” Artificial Organs pp. 704-706, Internet: http://www3.interscience.wiley.com/journal/121514553, 2008, [30 Jun 2009].
- [11] Gordon Giesbrecht and James A. Wilkerson. Hypothermia, Frostbite, and Other Cold Injuries. Seattle: Mountaineers Books, 2006.
- [12] “Membrane Oxygenators.” Perfusion Equipment. Internet: http://www.perfusion.com.au/CCP/Perfusion% 20Equipment/Membrane%20Oxygenators.htm, 2008 [30 Jun 2009].
- [13] J, H Schnöring Arens, F Reisch, JF Vázquez-Jiménez, T Schmitz-Rode, and U Steinseifer. “Development of a miniaturized heart-lung machine for neonates with congenital heart defect.” American Society for Artificial Internal Organs Journal[i/], vol. 54(5), pp. 509-13. Internet: http://www.ncbi.nlm.nih.gov/pubmed/18812743?ordinalpos= 3&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSum, 2008, [30 Jun 2009].
- [14] “AHA Open-Heart Surgery Statistics.” American Heart Association. Internet: http://www.americanheart.org/presenter.jhtml?identifier=4674, 2009 [29 Jun 2009].
- [15] Mark Z. Jacobson. Fundamentals of Atmospheric Modeling. New York: Cambridge University Press, 2005.
- [16] “Ready for action: The 17.5 kg heart-lung machine.” European Hospital Online. Internet: http://www.european-hospital.com/topics/article/2412.html, 1 Sep. 2007 [6 Jul. 2009].

